
Shoulder Clinical Reasoning for physiotherapy students
TL;DR
This shoulder decision flow helps students avoid a common clinical reasoning mistake: confusing a label with an explanation.
Tests such as painful arc, Hawkins–Kennedy, cuff testing, or biceps tests can help organise the presentation, but they do not by themselves explain what is driving the patient’s problem. First, decide whether the patient needs an ICD-level medical pathway or can be managed within an ICF physiotherapy framework. Then use the pattern checkpoints to record the presentation, but always continue to a contributor screen.
From there, map the likely contributors, such as the GH joint, AC joint, SC joint, scapulothoracic region, cervical spine, thoracic spine, and relevant psychosocial or behavioural factors. Rank the main drivers, form an ICF-based working diagnosis, treat the most relevant contributors, and reassess. In short: pattern labels help organise findings, but contributors should guide treatment.
Disclaimer
I am currently employed as a teacher and researcher at Hanze University of Applied Sciences. This post and the accompanying charts are intended as educational support material for physiotherapy students.
The material is not an official Hanze publication and should not be read as representing the formal views, policy, or curriculum position of Hanze University of Applied Sciences. Although I teach shoulder assessment and clinical reasoning within higher education, these charts are not presented as Hanze-specific curriculum documents.
The content reflects my own professional interpretation of shoulder clinical reasoning, based on my experience as a physiotherapist, manual therapist, teacher, researcher, and clinical supervisor. The charts have been written at a level intended to be useful for early-stage physiotherapy students, regardless of the university or programme in which they study.
Image use and licence
The images and charts in this post may be downloaded and shared for non-commercial educational use under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International licence.
This means that you may copy and share the images in teaching, student resources, presentations, and professional discussion, provided that:
- the images are shared unchanged;
- the use is non-commercial;
- proper attribution is given;
- a link is provided to the original source.
Suggested attribution:
Image/chart by Robert Goddard, Fysiotherapie Noorderbad. Used under CC BY-NC-ND 4.0. Original source: [insert link to this blog post].
Please do not present these images as official Hanze materials, and do not imply that they represent the formal position of Hanze University of Applied Sciences. They reflect my own professional interpretation of shoulder clinical reasoning and are shared as open educational support material.
For permission to adapt the images, translate them, include them in commercial material, or use them in a paid course or publication, please contact me first.
When assessing a patient with shoulder pain, it is tempting to move quickly from a positive test to a diagnosis. A painful arc, a positive Hawkins–Kennedy test, weakness on resisted testing, or pain during a biceps load test can all feel like they are “telling us what the problem is”.
But in clinical reasoning, these findings are only the beginning.
The key rule is simple:
A likely diagnosis is not the same as a causal explanation.
Why this flowchart matters
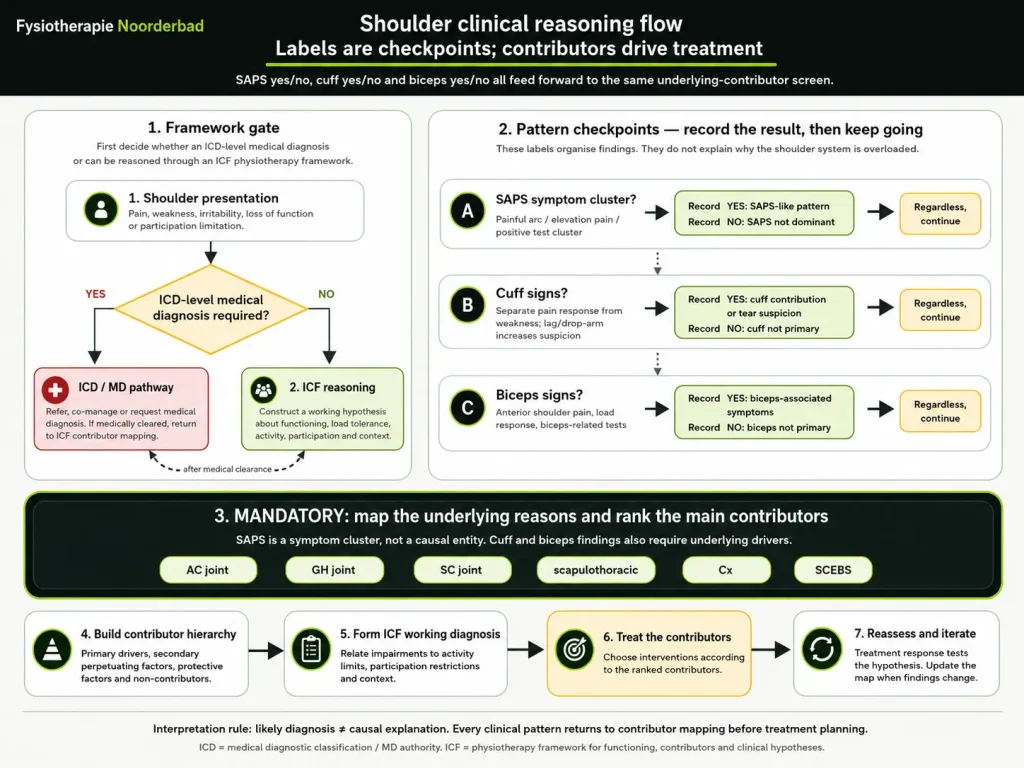
Step 1: First decide whether this is an ICD-level medical problem
Before building a physiotherapy hypothesis, first ask whether the patient needs a medical diagnostic pathway.
Is there suspicion of fracture, serious pathology, systemic disease, acute traumatic rupture, neurological compromise, or another condition requiring medical diagnosis or co-management?
If yes, the patient belongs on an ICD/medical pathway. That may mean referral, co-management, or requesting further diagnostic clarification.
If no, or once medically cleared, we continue with an ICF-based physiotherapy reasoning process.
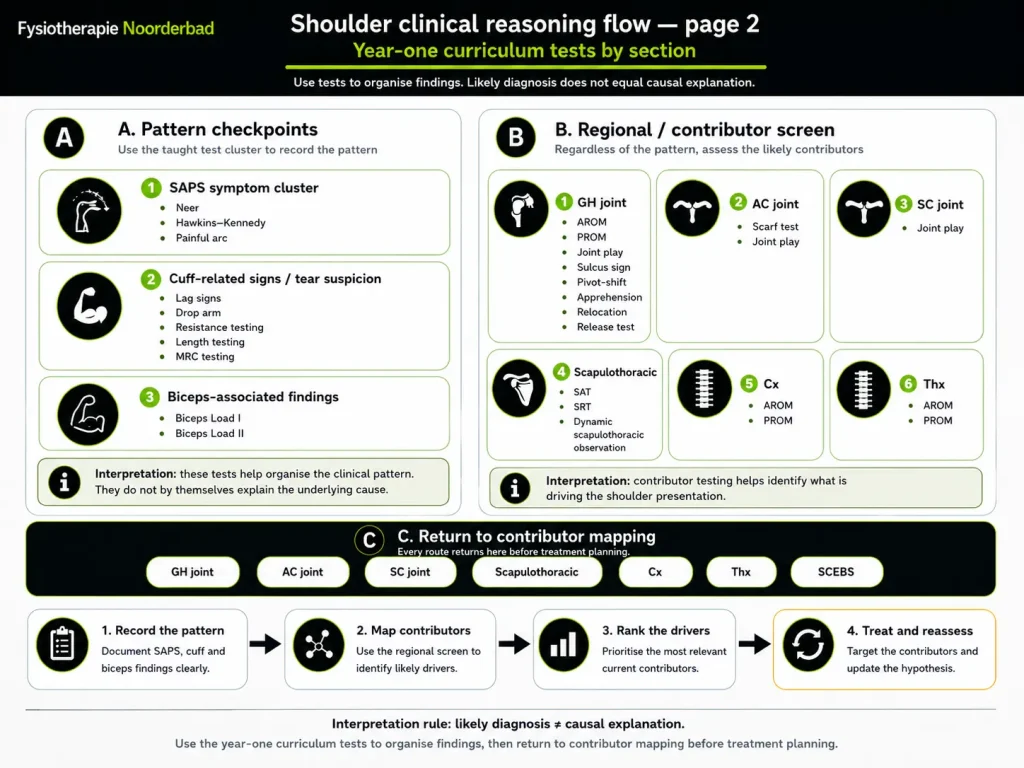
Step 2: Use pattern tests to organise the presentation
The first part of the shoulder assessment helps you organise the clinical pattern.
For example, the taught test clusters may help you record whether the presentation looks like:
SAPS-like symptoms, using findings such as Neer, Hawkins–Kennedy, and painful arc.
Cuff-related signs or tear suspicion, using lag signs, drop arm, resistance testing, length testing, and MRC testing.
Biceps-labral or SLAP-related suspicions, using tests such as Biceps Load I and II.
These labels are useful. They help us describe what we see.
But they do not explain what caused the shoulder to start hurting in the first place. Knowing which structure is potentially a source of nociception and knowing what is the causing/maintaining the problem are two different things.
That is the common reasoning error: treating the label as if it were the cause.
Step 3: Regardless of the label, map the contributors
Whether the patient appears to have SAPS-like symptoms, cuff-related signs, biceps-associated symptoms, or none of these clearly, the next step is the same:
Map the underlying contributors.
This means screening the regions and systems that may be driving the shoulder presentation, such as:
The glenohumeral joint, AC joint, SC joint, scapulothoracic region, cervical spine, thoracic spine, and relevant SCEBS factors.
A shoulder can be painful because of local tissue sensitivity, reduced load capacity, altered scapular control, cervical contribution, thoracic mobility limitations, training load, fear, sleep, stress, or a combination of several factors.
The clinical label helps us organise the findings.
The contributor map helps us decide what to treat.
Step 4: Build a contributor hierarchy
After testing, do not list every positive finding as equally important.
Clinical reasoning requires ranking.
Which finding is most relevant to the patient’s current problem? Which one seems to be a primary driver? Which is secondary? Which is simply present, but probably not clinically important?
A useful hierarchy might include:
Primary drivers, secondary contributors, perpetuating factors, protective factors, and non-contributors.
This hierarchy is more useful than a long list of positive tests, because it gives direction to treatment planning.
Step 5: Form an ICF working diagnosis
The ICF framework helps us move beyond tissue labels.
Instead of only saying “this patient has SAPS” or “this looks like a cuff problem”, we ask how the impairments relate to activity limitations, participation restrictions, load tolerance, and the patient’s context.
A better physiotherapy working diagnosis describes the patient’s actual clinical situation:
What is limited?
What is sensitive?
What is overloaded?
What is underprepared?
What needs to change for this person to function better?
Step 6: Treat the contributors, then reassess
Treatment should target the ranked contributors, not simply the diagnostic label.
If scapulothoracic control is the main driver, treat that.
If glenohumeral stiffness is dominant, treat that.
If cervical contribution is relevant, include it.
If load management is the main issue, modify loading.
If fear, sleep, stress, or beliefs are maintaining the problem, they must be part of the plan.
Then reassess.
Clinical reasoning is not a one-way street. Treatment response tests the hypothesis. If the patient improves, the reasoning becomes more plausible. If they do not improve, the map must be updated.
The main takeaway
Shoulder tests are not useless, but they must be used correctly.
They help us record patterns.
They help us organise findings.
They help us communicate what we have observed.
But they do not, by themselves, explain the cause of the patient’s problem.
For good clinical reasoning, remember:
Labels are checkpoints. Contributors drive treatment.
Try this: Next time you assess a shoulder, ask: ‘What’s the pattern?’ Then: ‘What’s driving it?’
Guideline check: where this flowchart fits with current evidence
This flowchart is a clinical reasoning aid, not a diagnostic calculator.
Current guidelines support the central message of this post: a clinical label should not be treated as a causal explanation. SAPS is described as a typical shoulder pain pattern, and its exact cause is not always clear. The NHG shoulder guideline also states that the exact anatomical place or cause of non-traumatic shoulder pain is usually not identifiable with certainty and often has no direct consequence for treatment.
There are also important limits.
First, the 2025 Dutch SAPS guideline does not require large clusters of special tests to diagnose SAPS. It recommends using a single test when the question is whether SAPS or rotator cuff rupture is more or less likely. In this post, test groupings should therefore be read as educational pattern-recognition checkpoints, not as diagnostic proof.
Second, the SAPS diagnostic-test guideline is narrower than this flowchart. It does not cover the full physiotherapy reasoning process, and it explicitly leaves cervical spine assessment and psychosocial factors outside that module. The contributor screen in this post should therefore be understood as a physiotherapy reasoning framework, not as a direct SAPS guideline algorithm.
Third, scapulothoracic findings require caution. Altered scapular movement may be clinically relevant, but dynamic scapular movement is difficult to measure reliably. Students should avoid presenting scapular control as a precise objective diagnosis. It is safer to ask whether scapulothoracic control appears symptom-relevant, modifiable, and useful as a reassessment marker.
So the guideline-safe interpretation is:
Use pattern tests to organise the presentation. Do not use them as proof of tissue causation. Use contributor assessment to build a treatment hypothesis. Use reassessment to test whether that hypothesis was useful.
The practical student rule remains:
Labels help organise the case. Contributors help guide treatment. Reassessment tests the hypothesis.
AI transparency statement
This post was developed with support from AI-assisted writing tools for drafting, editing, structure, and clarity. The clinical reasoning model, educational interpretation, final wording, and responsibility for the content remain my own. AI was not used as a substitute for professional judgement or guideline-based clinical reasoning. No personal patient data were used.