
Neurological conditions
One of the most confusing topics for my first year physiotherapy students is (peripheral) neurology. Especially the different conditions such as ALS, Guillain-Barré, Critical illness polyneuropathy etc. To be honest i totally get it, it is confusing, there are overlapping symptoms such as weakness, loss of sensation and wasting.
I decided to see if i could enlist the help of ChatGPT to help me create an overview for my students, to help clarify the main differences between these diseases.
When assessing this kind of thing I personally find it helpful to concentrate on what makes a disease unique or at least different. Once you have a good handle on what is unique or differentiating between diseases or disorders on certain key areas such as onset, symptoms or progression, it all becomes a lot easier.
Neurological conditions can present with weakness, sensory changes, reduced reflexes, muscle wasting, or functional decline. Although Guillain–Barré syndrome, peripheral polyneuropathy, ALS, and critical illness polyneuropathy can appear similar at first glance, they differ markedly in onset, underlying pathology, prognosis, and management. Understanding these differences helps clinicians recognise important patterns during assessment and clinical reasoning.
I would like to share some insights regarding four neurological conditions commonly encountered in neurological education and clinical practice.
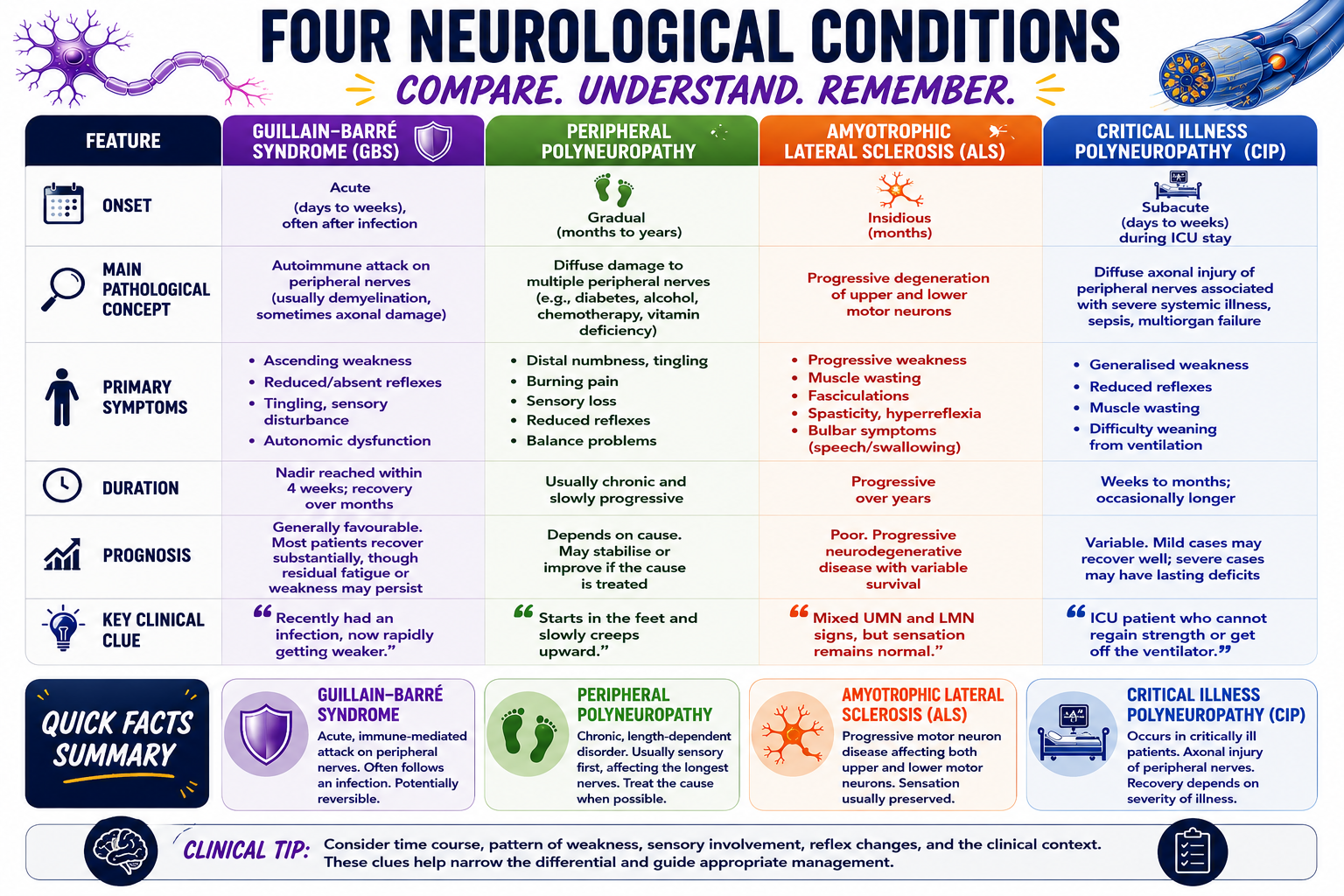
The infographic
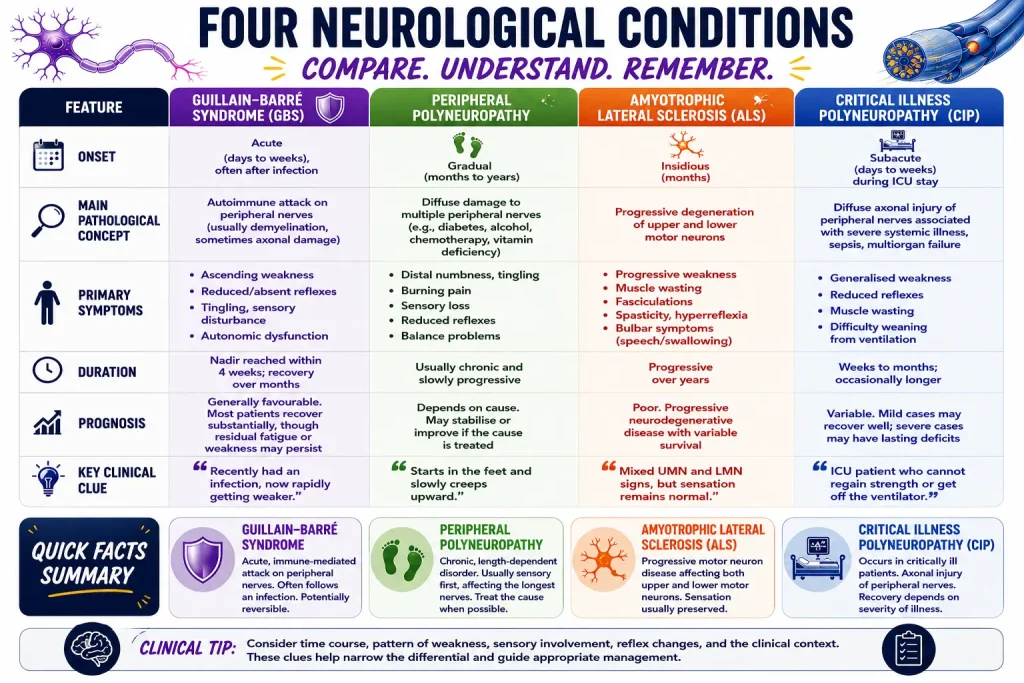
To download a higher quality version click here: Download high-res infographic neurological conditions
{kind=link}
Key Learning Points
- Guillain–Barré syndrome is an acute autoimmune attack on peripheral nerves that often follows infection.
- Peripheral polyneuropathy is usually a chronic, length-dependent disorder affecting the longest peripheral nerves first.
- ALS is a progressive motor neuron disease affecting both upper and lower motor neurons while generally sparing sensation.
- Critical illness polyneuropathy develops during severe systemic illness and is commonly encountered in intensive care settings.
Guillain–Barré syndrome
Guillain–Barré syndrome (GBS) is an acute autoimmune disorder of the peripheral nervous system that often develops one to six weeks after a respiratory or gastrointestinal infection. Through a process known as molecular mimicry, the immune system mistakenly attacks components of peripheral nerves, most commonly the myelin sheath but sometimes the axon itself. This disrupts nerve conduction, leading to rapidly progressive, typically ascending weakness, loss of reflexes, sensory disturbances, and occasionally autonomic dysfunction. Symptoms usually worsen over days to weeks before reaching a plateau, after which recovery begins as inflammation resolves and nerves remyelinate or regenerate.
Peripheral Polyneuropathy
Peripheral polyneuropathy refers to a group of disorders characterised by diffuse dysfunction of multiple peripheral nerves, usually affecting the longest nerves first. Common causes include diabetes, chronic alcohol use, chemotherapy, kidney disease, and vitamin deficiencies. The underlying pathophysiology involves metabolic, toxic, vascular, or inflammatory damage to nerve axons and/or myelin, resulting in impaired transmission of sensory and motor signals. Because the longest nerves are most vulnerable, symptoms typically begin in the feet and progress proximally in a “stocking-glove” distribution, causing numbness, tingling, burning pain, reduced reflexes, and impaired balance.
Amyotrophic Lateral Sclerosis
Amyotrophic lateral sclerosis (ALS) is a progressive neurodegenerative disease that affects both upper motor neurons in the brain and lower motor neurons in the brainstem and spinal cord. The exact cause remains incompletely understood, but proposed mechanisms include abnormal protein aggregation, glutamate-mediated excitotoxicity, oxidative stress, mitochondrial dysfunction, and neuroinflammation. As motor neurons degenerate and die, muscles lose their neural input, leading to progressive weakness, muscle wasting, fasciculations, spasticity, and hyperreflexia. Importantly, sensory pathways are usually preserved, so patients typically retain normal sensation despite severe motor disability.
Critical Illness Polyneuropathy
Critical illness neuropathy (CIN) is an acquired axonal neuropathy that develops in critically ill patients, particularly those with sepsis, multiorgan failure, prolonged mechanical ventilation, or systemic inflammatory states. The pathophysiology involves a combination of inflammatory mediators, microvascular dysfunction, metabolic disturbances, and direct axonal injury, which impair the function and survival of peripheral nerves. Patients develop diffuse weakness, reduced reflexes, muscle wasting, and difficulty weaning from ventilatory support. Unlike Guillain–Barré syndrome, the process is not primarily autoimmune but is a complication of severe systemic illness, and recovery depends largely on the severity of the underlying disease and the extent of nerve damage.
Summary of neurological conditions
| Feature | GBS | Peripheral Polyneuropathy | ALS | CIP |
|---|---|---|---|---|
| Onset | Acute (days to weeks) | Gradual (months to years) | Insidious (months) | Subacute (days to weeks) |
| Main Pathology | Autoimmune attack on peripheral nerves | Diffuse damage to multiple peripheral nerves | Progressive degeneration of motor neurons | Diffuse axonal injury (severe illness, sepsis) |
| Primary Symptoms | Ascending weakness, reduced reflexes, tingling | Distal numbness, burning pain, sensory loss | Muscle weakness, fasciculations, spasticity | Generalized weakness, muscle wasting, difficulty weaning from ventilation |
| Duration | Nadir at 4 weeks; recovery over months | Chronic, slowly progressive | Progressive over years | Weeks to months |
| Prognosis | Generally favorable | Depends on cause | Poor: median survival 3-5 years | Variable |
| Key Clue | Recent infection, rapidly weakening | Starts in feet, creeps upward | Mixed UMN/LMN signs, normal sensation | ICU patient, cannot regain strength |
⚠️ Watch Out For:
- GBS vs. CIN: Both can present with acute weakness, but GBS is autoimmune (often post-infection) while CIN is ICU-acquired (sepsis/MOF).
- ALS vs. Peripheral Neuropathy: Sensory sparing in ALS is a key differentiator—don’t miss it!
- Peripheral Polyneuropathy: Always check for diabetes, alcohol, or B12 deficiency as underlying causes.
Test Your Understanding
- A patient presents with ascending weakness, areflexia, and a history of diarrhea 2 weeks ago. Which condition is most likely?
- Which condition typically spares sensation despite severe motor disability?
- True or False: Critical illness polyneuropathy is primarily an autoimmune disorder.
(Answers: 1. GBS, 2. ALS, 3. False)